


In order to have a sequelae recognized by the SAAQ, the evidence must demonstrate, in general, that the existence of a causal link between it and the road accident is not only possible, but probable. The diagnosis of head trauma (“CBT”) is no exception to this rule.
 However, it is medically recognized that certain objectivable signs and symptoms that may occur after the accident, such as loss of consciousness, confusion or post-traumatic amnesia, may indicate the presence of permanent sequelae to the brain due to TBI.
However, it is medically recognized that certain objectivable signs and symptoms that may occur after the accident, such as loss of consciousness, confusion or post-traumatic amnesia, may indicate the presence of permanent sequelae to the brain due to TBI.
It will therefore be necessary to objectify these signs by health professionals, and this, in a contemporary way to your accident, since such damage to the brain does not usually begin to manifest itself several months after the accident, but a few hours or even a few days after it.
In addition, the symptoms associated with TBI tend to improve over time, not worsen, according to the medical literature. The courts will therefore be wary of symptoms that appeared too long after your accident, although the medical literature seems to be slowly evolving on this subject.
It may therefore be appropriate to consult the notes of paramedics who have intervened with you, for example, to determine if they have immediately noted symptoms of CBT, including:
- headache (headache);
- loss of consciousness;
- confusion;
- amnesia;
- dizziness;
- nausea;
- fatigue;
In addition, it may also be relevant to see your result on the Glasgow scale, as assessed following your accident. Indeed, this result will serve as a faithful indicator of your state of consciousness following your accident and can also indicate the presence of CBT. To this end, the extremes of 15/15 and 3/15 indicate respectively a state of perfect consciousness and a state of deep coma, or even clinical death, the latter of which may indicate the presence of TBI.
Other evidence of CBT include:
- the presence of amnesia of events preceding, surrounding or following the accidental event;
- a neurological deficit of central origin;
- a significant injury to the head or face (skull fracture, Le Fort fracture, facial mass fracture, deep lacerations to the head or face)
- a significant injury to the cervical spine (fracture or spinal cord contusion)
- clinical (Battle’s, raccoon glasses, etc.) or radiological signs of a skull fracture;
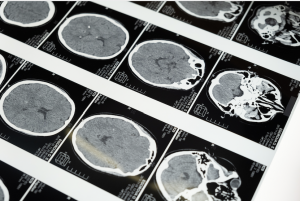
- a scan or magnetic resonance showing acute brain damage (contusion, axonal injury, hemorrhage, edema, etc.);
- a de novo convulsion post-accident.
Contact form
Please send us a message using the contact form below.
We will get back to you as soon as possible.
Identification of factors of poor prognosis
Other factors can give us clues about the extent of the head injury and the impact of this prognosis on the victim’s life, such as the mechanism of the accident, the severity of the brain injury, as well as personal, family and environmental factors.
With regard to the mechanism of the accident, there are in particular:
- the speed of the vehicle at the time of impact;
- the type of vehicle and the protections available
- the number of impacts;
- the presence of physical injury or death (evidence of the magnitude of the injury force);
- the condition of the person at the time of the accident (stiffening, alcohol intoxication, etc.);
- the distance at which the victim was thrown;
- and the nature of the impact on the ground.
Regarding the severity of the brain injury, it is necessary to see if there has been a positive neurological imaging or examination, a loss of consciousness of any duration, APT of more than one hour, any other injury added to the TBI, a Glasgow score of 13-14, an objective neuropsychological disorder, an episode of hypotension or neurological deterioration, the presence of an HSA or a skull fracture.
In terms of factors related to a premorbid individual, there are:
- age;
- medical history;
- personality style and personality compensation level;
- the quality of adaptive mechanisms;
- the presence of multiple stressors before the accident (usually twice as many);
- a history of learning disabilities;
- a poor level of education and socio-economic status.
Reaction factors include:
- an initial reaction that is out of proportion or that lasts more than a week;
- the presence of multiple post-concussion symptoms;
- maladaptive late reaction (PTSD)
- the accident or TBI is held responsible for all the difficulties experienced;
- a diagnosis of anxiety or depression
- the presence of stimulation elements.
With regard to family and environmental environments, there are:
- lack of family support;
- the presence of psychiatric problems within the family;
- an ill-adapted family response to the accident;
- unsatisfactory or difficult work;
- a family environment that places little value on work;
- poorly adapted social roles.
The importance of medical follow-up
We cannot stress enough the importance of follow-ups, whether in psychotherapy or psychiatry, social work, physiotherapy, occupational therapy, rehabilitation, etc.
The doctor who makes your diagnosis will also have to rule out all other possible causes that may explain your symptoms beforehand by ensuring, for example, in case of loss of concentration, that it is not attributable to ADHD or another disorder of the same nature.
Finally, it should be noted that the extent of the damage to your car can also be a good indicator of the strength of the impact felt during your accident, and therefore of the possibility that you have suffered a head injury.
If you have suffered a head injury following an automobile accident, do not hesitate to contact us to know your rights against the SAAQ.